Patient Rights Groups Are Learning the Wrong Lessons From ACT UP
These groups are invoking ACT UP’s legacy to push for further deregulation of the FDA. Here’s why they’re wrong.
I spent my 20s and 30s going to hospitals to visit friends and colleagues, and burying many of them. Their lives had been cut short by a cruel virus that was called a “death sentence” until effective treatments arrived in the middle of the 1990s to rescue those who had managed to survive that long. Close to 400,000 people in the United States alone perished from HIV/AIDS in the years up until around 1996, when what we called “highly active antiretroviral therapy” finally emerged.
I am one of the survivors. I found out I was HIV positive just before these powerful new medicines came on the scene. This morning, I took the pills I’ve been taking daily since 1996—the ones that keep me alive so I can tell you this story.
Back then, we were fighting for our survival against a government that didn’t care if we lived or died, and a society that had scorned gay men, people who use drugs, sex workers, and people of color before we had this disease, and hated us even more because this virus was now in our blood. But we refused to back down. We stood up for our right to human dignity, to life, to health. We also transformed the way the world thinks about the relationship between patients, people living with a disease, and healthcare providers, between federal agencies that support biomedical research and regulate the drugs we put in our bodies.
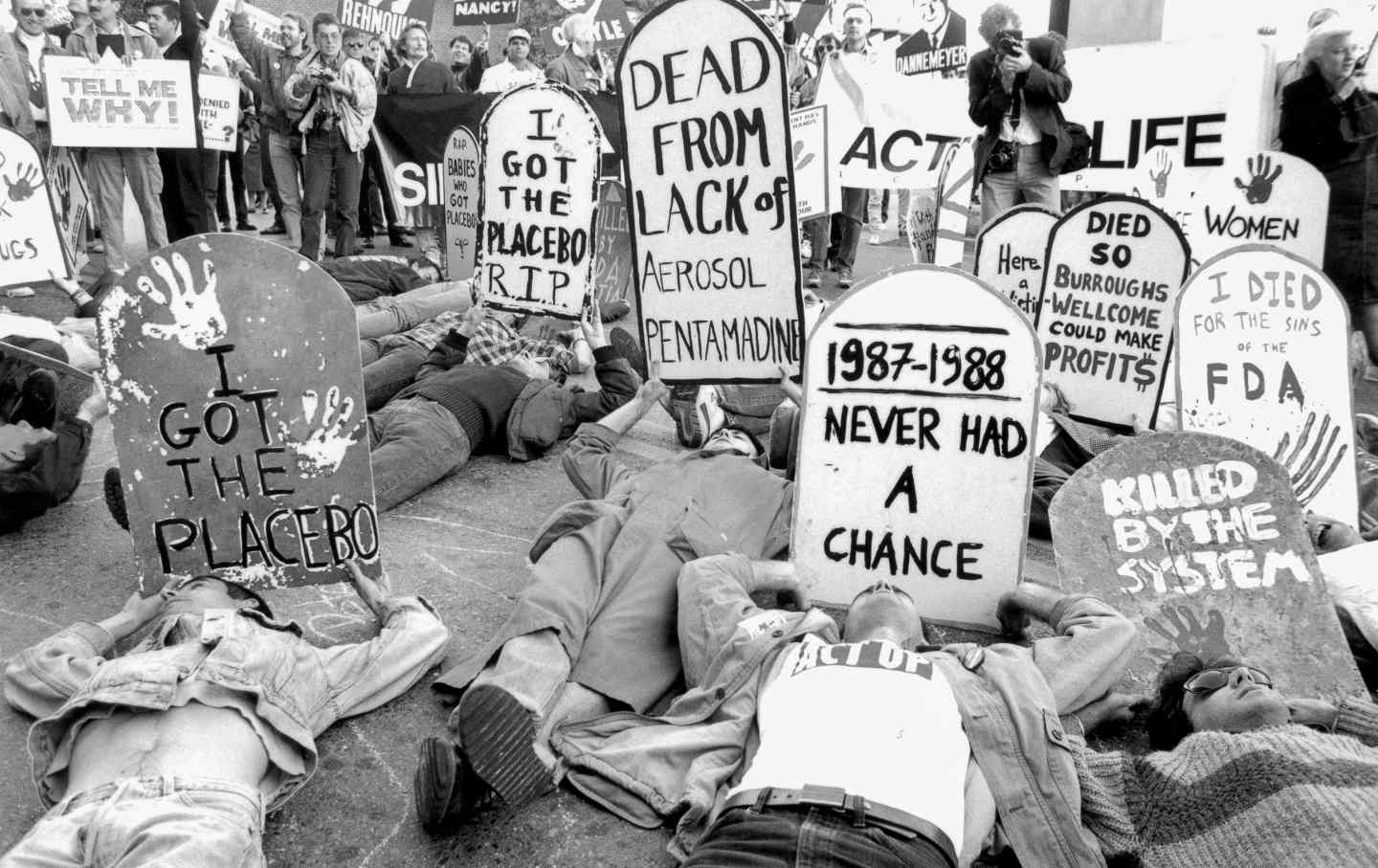
Many of you know the story of ACT UP (the AIDS Coalition to Unleash Power)—how, with direct action, protest, political savvy, and self-taught technical expertise, we took on the Food and Drug Administration, the National Institutes of Health, the drug companies, and the politicians.
It thus deeply pains me to see patient groups today—not for AIDS, but for a host of other diseases—distort what we were fighting for and use it for counter-productive purposes. Sometimes this stems from the sheer terror and desperation that I know so well, but it often emerges from thoughtlessness and outright collusion with drug companies. Their end goal appears to be to dismantle the FDA as we know it. As someone who fought alongside so many to change the way we develop and regulate drugs in the USA—including the role of the FDA—and who is only alive because of the fights that we won, I feel certain that these groups are making a terrible mistake.
There is no doubt that the FDA of the 1970s and ’80s was sclerotic, slow, and conservative. The tempo and trajectory of how we developed drugs—even ones not designed for public health emergencies such as the AIDS epidemic—were not fit for purpose. That’s why ACT UP “seized control of the FDA” in our first national action in 1988. The central motivating force of our campaign in those early years was to speed up the government’s regulatory pipeline so that we could actually use drugs that we hoped and believed could save our lives if the FDA approved them faster. This is the point that many of the patient groups today hark back to in invoking the work of ACT UP.
The flaw in their thinking, though, is that this is only part of the story—and in simply grabbing hold of the notion that “drugs into bodies” is the only thing that matters, they do a disservice to our legacy and to the future of patients today.
You see, for HIV back then, as for many diseases now, the lack of effective treatments wasn’t only about the FDA. It was also that the treatments going into the regulatory cascade simply did not work, or work well enough. That’s why, even as we pressured the FDA, we also fought ferociously to reform the way clinical trials were designed and conducted, forcing our way to a seat at the table with researchers and academics. We devoted considerable effort to the National Institutes of Health, figuring out how to jump-start biomedical research on HIV—to prime the pump, so to speak—and to get new ideas for treating this virus from the bench to the bedside.
At the FDA, while we pushed for proposals such as accelerated approval (yes, that was us), we also quickly realized that access to drugs alone was insufficient to save our lives. We needed rigorous evidence that they worked. We became experts in clinical trial design and were mentored by biostatisticians to help us understand how to evaluate these studies. We proposed the “parallel track,” a mechanism by which drug companies could offer new drugs for free to patients in “expanded access,” while the critical randomized, controlled studies to assess their efficacy continued. Several early drugs, such as ddI and d4T, were offered to tens of thousands of patients, while others enrolled in studies of the drugs as well. “Access AND answers” was our mantra.
One of the great regrets of my life is what happened next. Drug companies and the politicians who love them had been looking for years for ways to loosen the evidentiary requirements for approval of new drugs, and while they were a powerful force in DC, they needed something more, an emotional hook, a way to break through to turn the FDA into an even less sympathetic agency. The early ACT UP slogan, “the FDA is killing us,” was ready-made for the apostles of deregulation on the libertarian right in the late 1980s and early ’90s, and at its core, it still lingers in the way many talk about the FDA today. In fact, I would suggest it has been mainstreamed by powerful patient groups in the United States.
The truth is, the FDA—or at least the concept of it—isn’t killing us. But some patient groups may help to destroy the chance for us to get the FDA we need.
We get drugs more quickly onto the market in the US than ever before, faster than many peer regulatory agencies in other nations, but at the same time, we know less and less about what we put in our bodies and often pay more and more for drugs with dubious, unproven efficacy. I wrote about the follies of Alzheimer’s disease drug development a few months ago for this magazine, a calamitous situation driven in large part by patient groups and the drug manufacturer.
We’ve been seeing more and more of this lately. Drugs that have little evidence that they work are being pushed ahead by both corporate interests and patient groups parroting their talking points. Some of this is about alignment in motivations. Drug companies want to sell drugs and patients want to take them, but unproven remedies erode our faith in industry’s ability to deliver drugs that work and provide false hope to people suffering from life-threatening diseases. It’s a devil’s bargain that serves no one.
Popular
“swipe left below to view more authors”Swipe →We need the FDA to be more insulated from these forces. Instead, every few years, legislators offer bills that amount to death by a thousand cuts for the agency. The latest is the Promising Pathways Act, which offers “conditional approval” of new drugs, without even the need for the preliminary evidence that accelerated approval requires (i.e., some indication that biomarkers associated with real outcomes like disease progression or survival are moving in the right direction in early drug studies). The idea is that patients will get the drugs earlier, which may indeed be true, but it simply punts on the need for answers suggesting that data from registries or real-world evidence could substitute for rigorously designed clinical studies. Even then, companies get up to eight years to provide that data. This bill is being pushed by powerful patient groups and has the support of Democratic senators like Kristin Gillibrand and Raphael Warnock, who should know better.
The idea here is that patients don’t have time to wait for studies. I get it. Parallel track was built on this notion—give the drugs to thousands of patients for free while keeping the studies ongoing. But what we understood then, and is still true today, is that marketing approval is the only carrot the FDA has to incentivize the completion of those studies to give us the answers we need. Promising Pathways allows companies to market drugs with a promise akin to “the check is in the mail,” in terms of the studies that will tell us whether the drugs work or not.
Before we had an efficacy requirement for marketing approval established in the early 1960s, drugs in the US simply had to be regarded as safe to take to get sold in drugstores or prescribed by physicians. Yet we know from retrospective analyses of drugs from earlier in the 20th century that many of these “safe” drugs were not efficacious at all. In the FDA’s drug efficacy study implementation program, a third of all drugs approved under the previous regime were deemed ineffective. Perhaps, again, people will say, “Let me take my chances; let people and their doctors figure out if drugs work or not; perhaps we don’t need more than a patient registry or reports from doctors’ offices to adjudicate the effectiveness of new drugs.” This is the Yelp! version of drug regulation in the US, with weak evidentiary requirements and substandard study designs now in the ascendancy.
What harm could it do to establish this kind of system? The fact is that patients and doctors cannot evaluate the effectiveness of new drugs without rigorously designed studies. The history of American medicine is littered with the expert opinions of physicians who deemed certain drugs and medical procedures to be the standard of care for the treatment of various diseases. I did a little experiment on X, formerly known as Twitter, the other day—asking for examples in which this “expert opinion” turned out to be deadly. Dozens and dozens of examples poured in from physicians themselves and others about treatments that either turned out not to work or did more harm than good. In fact, there is a whole chapter in JAMA’s Users’ Guides to the Medical Literature on “Surprising Results of Randomized Trials” documenting this phenomenon.
We can reconcile the need for access and answers. Bringing back the parallel-track, large-scale expanded access programs before marketing approval would be critical to do. Right now, companies hold patients hostage on access—saying they cannot afford expanded access and faster approval is the only way to get their drugs. We can make studies larger and more inclusive, which has the virtue of enhancing the power in some settings to detect more modest treatment effects, but would also allow more people to enroll in them and done in the right way could diversify clinical trial enrollment.
And as hard as it is, we need some soul-searching among patient groups about the way in which they have eschewed the need for rigorous information about new drugs. (Again, the Alzheimer’s Association’s boosterism for aducanumab was a sorry tale.) However, some patient groups, like the National Organization for Rare Disorders are showing the way forward, mincing no words about proposals such as the Promising Pathways Act: “this legislation, by its own terms, would lower FDA’s approval standards, exposing patients to unsafe and ineffective medicines.” We also need to keep our eyes on the prize for all diseases, as this statement from the National Breast Cancer Coalition offers: “Drugs must be approved based on clinically meaningful outcomes rather than unvalidated surrogate endpoints and that we need more drugs that save or meaningfully improve patients’ lives, not simply more drugs.”
More from The Nation

A Civil Rights Veteran Revisits the Summer of 1965 A Civil Rights Veteran Revisits the Summer of 1965
The white college student supported Black voters in segregated Alabama, and began documenting the front lines of the voting rights fight, which locals continue to disregard.

Notes on Transsexual Surgery Notes on Transsexual Surgery
An abundance of plastic surgery is not a net good. But discussions over its morality would be better off viewing it less as unfettered desire and more as self-determination.

I Led the FDNY. Don’t Believe Elon Musk’s Nonsense About It. I Led the FDNY. Don’t Believe Elon Musk’s Nonsense About It.
Musk’s attack on the new FDNY commissioner proves he knows nothing about how modern fire departments work.

What Black Youth Need to Feel Safe What Black Youth Need to Feel Safe
Young people are facing a mental health crisis. This group of Cincinnati teens thinks they know how to solve it.

Trump’s Death Eaters Are Coming for Our Kids Trump’s Death Eaters Are Coming for Our Kids
After taking countless lives around the world, RFK Jr. and his ghoulish compatriots want American children to suffer too.

The Supreme Court Just Held an Anti-Trans Hatefest The Supreme Court Just Held an Anti-Trans Hatefest
The court’s hearing on state bans on trans athletes in women’s sports was not a serious legal exercise. It was bigotry masquerading as law.

